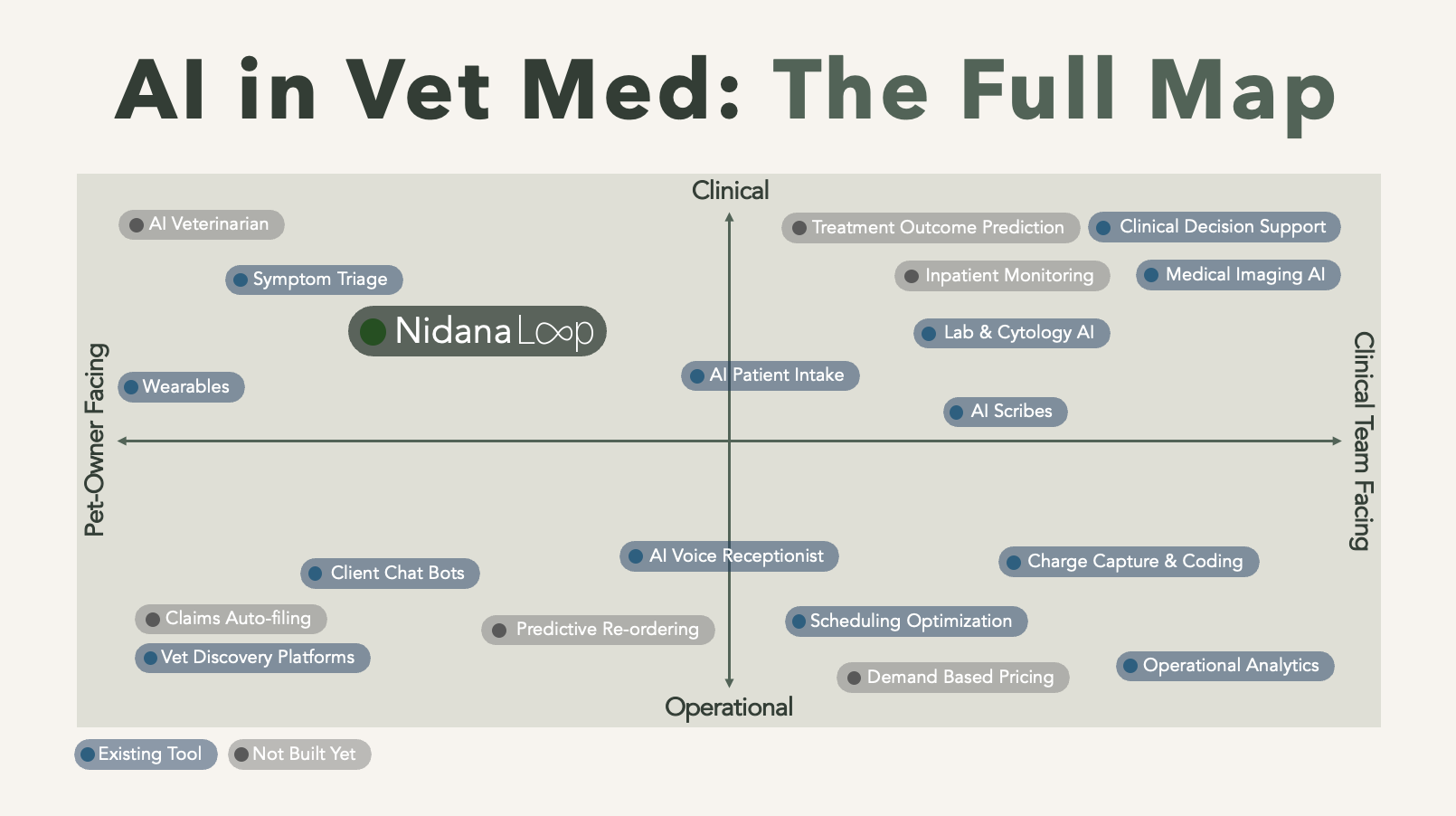
AI has moved through veterinary medicine faster than almost anyone has had time to track. A few years ago it was a curiosity. Today it writes up consults, reads radiographs, answers the phones, and sizes up symptoms in an owner's app, with new tools arriving faster than any one person can follow. | So here is the full picture in one place: every kind of AI now working in a veterinary practice, sorted by the job it does and who it serves. Four minutes from now you will be able to place almost any tool you come across, and you will know where things actually stand. | How to read the map | Andreessen Horowitz has a clean way of sorting AI in human healthcare: by the "job to be done," along two questions and this can be adapted very well to veterinary medicine. | Clinical or operational? Clinical work touches the medicine and the animal's health, so the bar it has to clear is trust and judgment. Operational work runs the business, so the bar is simply time and money. For your team, or for the pet owner? Team-facing tools give your people leverage inside the building. Owner-facing tools reach past the front door, to the client and the patient at home.
| Then one more question, the one most lists skip: is it actually AI, or ordinary software wearing the label? Real AI perceives, predicts, or generates. It reads an image, understands speech, holds a conversation. A scheduled reminder text is automation, not intelligence. Keep that filter on as you read, because most of the crowded categories do not pass it. | | | Clinical AI, for your team | This is where the genuine tools cluster, and where they differ most from one another. The clearest way to see them is to rank them by how much clinical judgment they actually take on. | It captures. The AI scribe. Listens to a consult and writes the medical record. The intelligence here is speech and language, not medicine: it documents what was said and diagnoses nothing. It is the most crowded corner of vet AI, because notes are the biggest time sink in a clinician's day and the job is low-risk and easy to define. In human medicine, clinicians spend close to two hours on the record for every hour with patients, and vets carry their own version of that tax. It interprets. Diagnostic and imaging AI. Computer-vision models read radiographs, cytology and blood smears and flag what looks abnormal. This is AI making a clinical inference, a far harder and higher-stakes job than transcription, with a real validation and liability bar behind it. It suggests. Clinical decision support. Surfaces differentials, dosing and drug interactions at the point of care. The newest and least settled of the three, and the one where quality varies most.
| A scribe and an imaging model both get sold as "clinical AI," but one writes down what you said and the other tells you what it sees inside an X-ray. Hold them to completely different standards. |
|
| | Operational AI, for your team | The phones are the most visible piece, but they are not the whole quadrant. | AI voice agents, on reception. Answer calls around the clock, triage the urgent from the routine, and book appointments without tying up the front desk. Charge capture and coding. Read the record to flag missed charges and the codes that fit, closing the gap between work done and work billed. Scheduling and no-show prediction. Forecast which appointments are likely to fall through and reshape the day around it, rather than just storing the calendar. Demand forecasting. Predict what the shelves will need before they run short, instead of reordering on a fixed rule. Practice intelligence. For groups, read a practice's own data to surface patterns and anomalies across locations that no one has time to find by hand.
| One caution, because the label is slippery here: most of these run on top of ordinary software, the PIMS, the billing and scheduling systems, with an "AI" feature bolted onto one corner. The intelligence is the model that predicts or reads, not the system it sits on. Most are also younger and less proven than the scribe, so test the demo against daily reality before you buy. | What the genuine tools in these first two zones share is leverage. They take the rote work, the typing, the phone tag, the chasing of numbers, so a profession that is short on people and heavy with burnout can spend its scarce hours where a person is actually needed. | | Operational AI, for the pet owner | Crowded with products, thin on real AI, because out here the label is loosest. | Client-facing chatbots and messaging. The text cousin of the AI receptionist: assistants on a clinic's website or inbox that answer routine questions, book visits, and help sort or draft replies to incoming messages. Where it is genuinely conversational, it is real AI.
| Almost everything else here is automation, not intelligence. Reminders, online booking, membership plans and review requests predate this wave by a decade. A reminder is a scheduled message, however well timed, and a booking page is a form. Useful, but do not let the "AI" on the box fool you. | | The empty corner | Put the filter and the two axes together, and one quadrant is nearly bare: clinical AI, the medicine, aimed at the pet owner. The little that lives there is reactive or passive. Symptom checkers wait for the owner to begin, then rate urgency and point them to a professional. Wearables report numbers and leave the reading to someone qualified. | It is worth being honest about why. In every other corner, a trained professional sits between the AI and any real consequence. The vet reads the scribe's note before signing it, weighs the imaging flag against the patient in front of them, takes or leaves the decision support. The AI advises and a human decides, which is what keeps it safe. Point that same clinical AI straight at the owner, with no clinician in the loop, and the risk changes entirely: the technology would be making medical judgments for someone who cannot catch its mistakes, and it is not good enough yet to be trusted with that. Even in human healthcare, the tools that reach patients directly are mostly triage and reminders, almost never diagnosis or treatment. | It is also the corner with the most still ahead of it. The boldest version, an AI an owner could consult directly, is the high-risk frontier from a moment ago, and nothing trustworthy enough exists yet. The safer ways in are narrower for now, and there is room for many of them. One is post-discharge monitoring: checking on a patient through the days that decide a recovery, watching for what tends to go wrong once they are home. Human medicine treats it as a normal part of care. Veterinary medicine, for all its new tools, has mostly not built the equivalent. | Nidana Loop sits here. It is post-discharge monitoring for veterinary practices: it reaches the owner by phone and text after a visit, asks the questions that fit the case, and hands the clinic a clear read on which patients are fine and which need another look. The rest of this map is about making the visit better. This part is about everything that happens after it. Curious what that looks like for your clinic? Book a demo. | Practice Forward is published fortnightly for vet teams. If this was useful, forward it to someone who would find it useful too. Read Online. |
|